

By Mike Wong, Registered Physiotherapist, MScPT, BHK | EastWest Physiotherapy in Burnaby, BC
That dull, aching pain behind and/or around your kneecap when you climb stairs, squat down, or getting up after sitting for too long? The condition is called Patellofemoral pain syndrome (PFPS) or Patellofemoral Syndrome (PFS), often called runner’s knee, and is one of the most common causes of knee pain we see at EastWest Physiotherapy in Burnaby. With the right treatment plan blending the latest evidence based research, state of the art physiotherapy modalities, and our Therapist’s expertise, many of our clients can get lasting relief quickly.
What Is Patellofemoral Pain Syndrome (PSPS)?
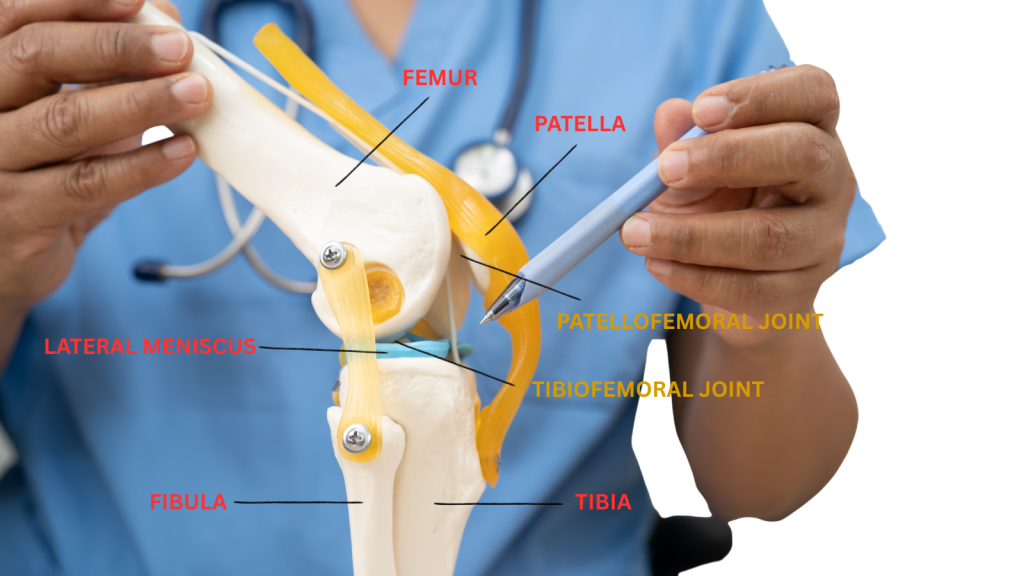
Your kneecap (the patella) sits in a groove at the front of your thigh bone (femur). Whenever you bend and straighten your knee, the patella slides up and down, in and out, in that groove in a particular manner. When the kneecap doesn’t move along the groove properly, the forces running through the joint can exceed what the surrounding tissues can handle. As a result, pain, swelling and the inability to bend and straighten your knee comfortably may show up.
The cartilage on the back of the kneecap isn’t what hurts directly, since cartilage has no nerve endings. The real sources of pain are the soft tissues around the joint: the synovial lining, the fat pad, the connective tissue on the side of the kneecap, and the bone itself. This is why pain can be so variable.Some people feel it constantly, while others only when going downstairs or getting up from a sitting position after a long meeting.
Up to 45% of young, physically active people experience patellofemoral pain at some point. It’s the most common knee complaint in runners.
Common Symptoms to Watch For
Patellofemoral pain doesn’t always feel the same from person to person, but these are the most common signs:
- Aching or sharp pain around or behind the kneecap
- Pain that gets worse going downstairs, squatting, or landing from a jump
- Stiffness or pain after sitting for a long time with knees bent (sometimes called “movie sign” or “theater sign”)
- A grinding or clicking sensation when bending and straightening the knee
- Pain that flares up with high-impact activities on the knees such as running, hiking, volleyball or basketball
Squatting is actually the most reliable test Physiotherapists use to identify patellofemoral pain. If squatting reproduces your knee pain in and around the kneecap area, there’s a good chance PFPS is involved.
What Actually Causes It?
Patellofemoral pain is caused by a multitude of factors. Research has shifted away from the old idea that it’s purely a kneecap tracking problem. Today, we understand it as a condition driven by several overlapping issues:
Muscle Weakness
Weakness in the quadriceps (especially the inside quad muscle called the VMO – Vastus Medialis Oblique) and the hip muscles, particularly the hip abductors and external rotators, is consistently identified as a major contributing factor. When these muscles aren’t doing their job, the kneecap may get pulled off course and the patellofemoral joint takes on more stress than it should. The weakness of the muscles above and below the knee joint affects the overall alignment of the leg.
Too Much Load, Too Fast
Feeling great and so motivated to get started in your training? Training errors are a leading trigger: increasing running mileage too quickly, jumping into a new sport, or going from sedentary to highly active without building up gradually. The joint simply can’t adapt fast enough. Repetitive stress to the same structures combined with inadequate rest periods creates microtrauma and injuries.
Movement Patterns
How you move matters. Runners who land heavily on their heel, people who let their knees cave inward and too far forward during squats, or those whose hips drop to one side when walking: all of these patterns increase the load on the patellofemoral joint over time. Combined with repetitive movements and activities like running can repeatedly stress the joint – death by a million cuts! When starting a new activity, it is wise to seek out guidance from our therapists to ensure you are moving properly, have good posture, and identify any muscle imbalances that may be causing dysfunctional movement patterns.
Pain System Sensitization
In patients with long-standing, chronic knee pain, the nervous system can become sensitized as the pain signals get amplified beyond what the tissue damage would normally explain. This is called central sensitization, and it’s one reason some people continue to hurt even after their knee looks fine on imaging. Psychological factors like anxiety, fear of movement, and catastrophizing can also intensify symptoms and slow recovery. The brain amplifies any sensation around the knee joint. This can perpetuate the cycle of pain → too much rest → deconditioning →use of the knee a bit → pain again, etc.
Anatomy
Some structural features, like a high-riding kneecap on the femur (patella alta) or a shallow femoral groove, can increase vulnerability of kneecap tracking issues. This is something that you cannot control, you are born with it. However, many people with these features never develop pain, while others with “normal” anatomy do. Structure alone doesn’t tell the whole story.
Who Gets Patellofemoral Pain?

PFPS affects people of all ages, but it’s most common in active teens and young adults. Women who are physically active are more susceptible than men in similar activity levels. Interestingly, young women who play multiple sports are at lower risk than those who specialize in a single sport; repetitive, one-dimensional loading patterns are harder on the joint than varied movement.
Beyond athletes, people in physically demanding jobs; construction, warehousing, and nursing face higher patellofemoral stress due to repeated squatting, kneeling, and stair climbing. Even desk workers aren’t fully protected: prolonged sitting with knees bent can aggravate an already sensitive joint.
How We Treat It at EastWest Physiotherapy Burnaby
At EastWest, we take an integrated approach that combines the strongest evidence-based Western rehabilitation techniques with complementary time-tested Eastern methods. No two people get the same plan, because no two knee problems are exactly alike.
Here’s how we approach patellofemoral pain:
Exercise Therapy
The foundation of every treatment plan. Hip and quad strengthening has the strongest evidence of any PFPS intervention. Our Physiotherapists will provide you a structured exercise program, ensuring proper technique and form, and the right progressions at the appropriate time.
Manual Therapy
Our Therapists will use hands-on joint mobilization techniques of the patella and surrounding structures, and soft tissue work to restore movement and reduce pain. Therapist assisted stretching of tight musculature around the hips, knees and ankle joints can also help.
Therapeutic Taping
Research showing patellar taping (McConnell technique) combined with exercise provides meaningful short-term pain relief, as the patella is encouraged to track optimally in its groove.
Acupuncture
May be used as part of a broader plan to support pain management and tissue recovery, not as a sole treatment technique for patellofemoral pain syndrome.
IMS / Dry Needling
Targets and effectively releases tight or overactive muscles around the knee and hip joints, contributing to poor movement patterns around the knee.
Electrotherapy
Supports tissue healing and pain modulation in the early stages of treatment. Various electrotherapeutic modalities including ultrasound, interferential, microcurrent, and traebert currents may be used to decrease symptoms immediately.
Exercise: The Most Important Part

The research is clear that supervised exercise targeting the hip and knee is the single most effective treatment for patellofemoral pain. The American Physical Therapy Association (APTA) recommends a combination of posterior hip and quadriceps exercises, things like single-leg squats, step-downs, lunges, and hip exercises with resistance bands. High volume training is effective. Three sets of 30 or more repetitions, three times per week, produces better results than lower-intensity programs.
Both weight-bearing and non-weight-bearing exercises work, and research shows benefits lasting up to five years when done correctly. The key is doing them consistently and gradual progressive loading, not just doing a few random exercises from a YouTube video.
Taping: Helpful, But Not on Its Own

Patellar taping, more importantly the McConnell technique, reliably reduces pain in the short term when used alongside exercise. This makes it a useful tool early in treatment when pain is limiting your ability to exercise effectively. On its own, taping doesn’t change the underlying problem because it is a muscle imbalance and weakness issue. When taping is paired with a solid exercise plan, it can get you moving sooner with less pain and discomfort.
Foot Orthotics

If your foot rolls inward (overpronation) when you walk or run, prefabricated foot inserts can reduce patellofemoral joint stress in the short term. Custom orthotics aren’t shown to be better than a well-chosen off-the-shelf insert, so our Physiotherapists can help you figure out the simplest effective solution.
Load Management
Especially for adolescents and athletes, managing how much load the knee takes is just as important as which exercises you do. We help you modify your activities intelligently, not by stopping everything, but by adjusting what you do and how much, then building back up with a clear plan.
For Runners: Gait Retraining
If your knee pain started with or is worsened by running, gait retraining can make a real difference. This includes increasing your step rate (cadence) to shorten stride length, transitioning away from a heavy heel strike, and managing weekly mileage. Running softer by reducing the impact forces your body absorbs with each step can measurably lower the stress on the patellofemoral joint.
What About Acupuncture for Knee Pain?
At EastWest Physiotherapy, acupuncture is one of the tools in our integrated toolkit, and we’re upfront about what the evidence says. Acupuncture shows benefit over no treatment for patellofemoral pain, but in head-to-head trials, it doesn’t clearly outperform a sham (placebo) procedure. This tells us there is a real benefit and part of it comes from the therapeutic relationship, relaxation, and neurological effects rather than needle placement alone.
We use acupuncture as part of a broader plan, not as a standalone treatment. In our experience, when acupuncture is paired with exercise, manual therapy, electrotherapy and individualized advice, it can support pain management and help patients engage in rehab more comfortably.
How Long Does Recovery Take?
This depends on how long you’ve had the problem, how active you are, and how consistently you follow your program. Most people with mild to moderate PFPS notice meaningful improvement within six to eight weeks of starting a structured exercise program. Some take longer, especially if the condition has been present for months or if there are signs of central sensitization or psychological contributors. Because of the variables in our clients, from age, overall health, activity levels, weight, attitude towards rehabilitation, we take treatment, prevention and long-term load management seriously from day one. Some of our clients resolve their patellofemoral pain in a few sessions, while others may take a bit longer.
Frequently Asked Questions
Is it ok to keep exercising if I have patellofemoral pain?
In most cases, yes, but you need to modify what you do rather than stopping completely. Complete rest rarely speeds up recovery and can make things worse by weakening the muscles that support the knee. The goal is to find a level of activity that doesn’t significantly increase your pain, then build from there. A physiotherapist can help you figure out exactly what “modified activity” looks like for your situation.
Do I need imaging (X-ray/MRI/Ultrasound) to diagnose patellofemoral pain?
Usually not. Patellofemoral pain is a clinical diagnosis based on your symptoms and a physical assessment. Imaging can be helpful to rule out other conditions like a stress fracture, ligament or cartilage injury, but X-rays and MRIs often show changes that are completely unrelated to your pain. An experienced physiotherapist can typically identify PFPS through your history and a hands-on exam.
What is the difference between patellofemoral pain and chondromalacia?
Chondromalacia refers to softening or breakdown of the cartilage on the back of the kneecap. It’s often used interchangeably with patellofemoral pain, but they’re not the same thing. Cartilage has no nerve supply, so chondromalacia itself can’t directly cause pain. Many people with significant cartilage changes have no pain at all, while others with no visible cartilage damage have severe symptoms. The treatment approach is similar regardless of whether chondromalacia is present.
Will my knee pain come back after treatment?
Research shows that exercise therapy can provide lasting benefits for at least five years. The key is building enough hip and knee strength, maintaining good movement habits, and avoiding the training errors that triggered the problem in the first place. People who only rely on passive treatments without strengthening are more likely to see their symptoms return. That’s why we always make long-term strength and movement education central to every treatment plan at EastWest Physiotherapy.
Does EastWest Physiotherapy Burnaby accept ICBC and WorksafeBC claims?
Yes, we accept ICBC claims for motor vehicle accident injuries and WorkSafeBC claims for workplace injuries. If your knee pain started or worsened following an accident at work or in a vehicle, you may be covered. Contact us at (604) 398-2936 to discuss your situation and we’ll help figure out your coverage options.
Ready to Get Your Knee Feeling Better?
Our Burnaby physiotherapy team combines evidence-based exercise rehab with proven Eastern techniques like acupuncture and cupping to create a plan that actually works for your knee, not just a generic protocol. One-to-one care, private treatment rooms, and real results.
About the author:
Mike Wong, MScPT (University of Alberta), BHK (Exercise Science) (UBC) is a Physiotherapist in Burnaby, BC and specializes in Orthopedic Physiotherapy, Acupuncture, Dry Needling and has a special interest in traditional Eastern Medicine treatment techniques.