TMJ Pain and Ear Fullness, TMJ Pain and Tinnitus - Is There a Link?
When you have issues with your TMJ such as arthritis, a trauma, a sprain or strain, or an irritation due to tight muscles and clenching, this leads to symptoms such as pain, clicking, head and neck pain, headaches, and inflammation. The TMJ is very close to the 3rd branch of the trigeminal nerve (V3). When your TMJ is irritated and inflamed, it can affect this nerve as the structures are very close together. This is how TMJ pain can cause issues such as ear fullness, and tinnitus.
How do TMJ issues cause ear fullness?
TMJ pain and ear fullness is quite a common report. Based on a meta analysis in 2017, it showed that an average of 75% of those with TMJ disorders experience ear fullness.
What could be causing this? The third branch of the trigeminal nerve supplies muscles of chewing, as well as the muscles that open and close the eustachian tube. These muscles are: the masseter, temporalis, pterygoid muscles, digastric muscle, mylohyoid muscle, the tensor veli palatini, and the tensor tympani. When the TMJ is irritated and inflamed and affects the trigeminal nerve, it can affect the function of any of the muscles listed above, including the tensor veli palatini.
The tensor veli palatini muscle helps open and close the Eustachian tube, allowing the middle ear to drain fluid into the nasopharynx. When the function of this muscle is interrupted, for example, due to inflammation of the trigeminal nerve, the Eustachian tube may not open properly. This will not allow the fluid in the inner ear to drain, causing symptoms like ear fullness, pressure, muffled hearing, and possibly temporary hearing loss.
Simply put, TMJ pain causes irritation to the trigeminal nerve, which interrupts the function of the tensor veli palatini muscle, which leads to ear fullness.
How do TMJ issues lead to tinnitus?
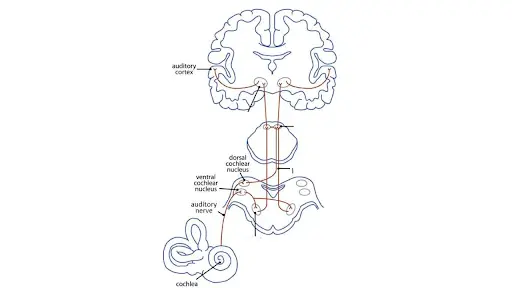
To understand tinnitus and TMJ issues, we need to understand how sound is processed in our brain. When a soundwave reaches our ear, it creates vibrations in the hearing organs of the inner ear. These vibrations are changed into electrical signals and travel through our cochlear nerve in the inner ear to the cochlear nucleus in the midbrain. The signal then moves up to the auditory cortex of the brain where we hear the sound.
There are two parts of hearing sound – we are able to hear the sound itself, and sense where the sound is coming from. This special ability uses our ears, and sensory information from our face, head, and neck. You may think that the cochlear nucleus is only for auditory information, but it receives information from other sensory pathways such as the trigeminal nerve. The trigeminal nerve carries sensory information from the face and jaw, and this extra input allows our nervous system to locate where sound is coming from.
For example, if you hear a sound but can’t locate it, you will immediately turn your head to see if you can find it. Our brains will receive auditory information to see if the sound is getting louder, and sensory information of what position your head and neck is to try and locate the source of the sound. This is one example of how our sensory and hearing system interact with each other.
Another clear example of how touch and sound affects each other is a simple, well known experiment called the “parchment skill illusion”. A researcher records the sound of your hands rubbing together, and replays it back to you at different frequencies while you continue rubbing your hands. If the sound is played at a higher pitch, you will feel as if your hands are dry, rough, and crinkly – like parchment paper. If the sound is played at a lower pitch, you will feel like your hands are soft and smooth. Sound affects touch (parchment skill illusion), and touch affects sound (locating sounds with turning your head and neck).
So now that we know all this background information, let’s go back to the original question of: How does my TMJ issue cause tinnitus?!
As you know, the trigeminal nerve sits very closely to the TMJ, and if the TMJ is irritated, it can also irritate that nerve. The extra nerve stimulation from pain, tension, and inflammation sends extra signals to the cochlear nucleus changing how sound is processed, and as a result – tinnitus. In these scenarios, you will notice that your tinnitus can change in pitch and volume depending on your movements, or muscle tension in the face, neck, jaw, and head.
What Can I Do About It?
To settle the symptoms of tinnitus and ear fullness, you need to settle down anything that is overstimulating your trigeminal nerve. Some things to address:
Stress
Manage your stress levels through methods such as meditation, deep breathing, yoga, journaling, or simply speaking with a trusted friend or family member. High levels of stress can increase muscle tone in the head, neck, and jaw region.
Clenching/ Grinding
Use mouth guards at night if you are aware of grinding at night. A mouthguard can help reduce the forces and impact at the TMJ. Grinding and clenching tightens the neck and jaw muscles worsening TMJ issues.
Dehydration
Muscles need proper amounts of water and electrolytes to contract and relax. Lack of water can upset the electrolyte balance and cause muscle cramps, tightening, and pain.
Posture
Maintaining good posture is important in preventing TMJ issues. A head forward position, or rotated head will affect the positioning of the TMJ and cause misalignments in the joint. Take notice how your posture affects your ear fullness and tinnitus. If you notice that the pitch or volume of the tinnitus changes with positional changes, that’s evidence that sensory information from your neck, face, or shoulders are affecting your tinnitus
Hot/cold compress
Heat is useful to help relax tight muscles of the jaw, neck, and shoulders. Using ice, on the other hand, can help settle inflammation at the TMJ if you have obvious swelling, redness and inflammation.
Massage
Self massage muscles that affect the TMJ. This includes muscle surrounding the jaw, the head and neck, and the upper trapezius. Keeping these muscles at an optimal length will prevent joint misalignment. If you notice that your tinnitus or ear fullness changes after a massage, it is evidence that extra sensory information from those muscles are affecting your tinnitus and ear fullness.
Avoid Hard and Chewy Foods
Eating hard and chewy foods work the muscles excessively which can irritate the TMJ. Again, notice if your tinnitus or ear fullness changes after working these muscles.
Medications
If needed, check with your doctor to see if antiinflammatories or muscle relaxants can help you decrease inflammation and relax tight muscles of the neck and jaw.
Self- Acupressure
ST6 (Stomach 6)
This point is used for any issues of the jaw, face, and teeth.
To locate this point:
ST7 (Stomach 7)
This point is useful for issues of the ear, jaw, and teeth. It is also very close to the trigeminal nerve, so if this spot is very sensitive, sore, or inflamed, make sure you keep the pressure gentle.
To locate this point:
GB20 (Gall Bladder 20)
This point is useful for issues of the head, neck, and eyes. Issues with the TMJ will usually involve the head and neck muscles, and this acupressure point can help release tension and stiffness in these areas.
To locate:
Li4 (Large Intestine 4)
This point is useful for a wide variety of conditions affecting the head and face. This can include headaches, sinus pain, teeth pain,and inflammation or infections of the head and face.
To locate:
Hopefully this article helps you understand what is causing your ear fullness and tinnitus. If you have any questions, feel free to reach out to one of our Burnaby Physiotherapists at EastWest Physiotherapy!
References:
Shore, S. E. (2011). Plasticity of somatosensory inputs to the cochlear nucleus: Implications for tinnitus. Hearing Research, 281(1-2), 38-46. https://doi.org/10.1016/j.heares.2011.05.001
Porto De Toledo, I., Stefani, F. M., Porporatti, A. L., Mezzomo, L. A., Peres, M. A., Flores-Mir, C., & De Luca Canto, G. (2017). Prevalence of otologic signs and symptoms in adult patients with temporomandibular disorders: A systematic review and meta-analysis. Clinical Oral Investigations, 21(2), 597–605. https://doi.org/10.1007/s00784-016-1926-9